
Translate this page into:
An unusual synchronous association of chronic myeloid leukemia with carcinoma tongue

*Sajal Goel, Department of Clinical Oncology, Delhi State Cancer Institutes, Dilshad Garden, Delhi, India. sajal.goel@yahoo.com
-
Received: ,
Accepted: ,
Abstract
Synchronous association of solid tumors with chronic myeloid leukemia (CML) is rare and only two cases had been reported till date. To the best of our knowledge, its association with head and neck carcinoma is being reported for the 1st time. The patient presented with a primary lesion in the right lateral margin of tongue and a blood picture diagnostic of CML. He was treated conservatively and kept on follow-up.
Keywords
Carcinoma tongue
Chronic myeloid leukemia
Synchronous
Unusual

INTRODUCTION
Synchronous malignancies have an incidence rate between 0.73% and 11.7%.[1,2] The only two cancers reported synchronously with chronic myeloid leukemia (CML) are stomach and breast.[3,4] Synchronous association with head and neck carcinoma is being reported for the 1st time. Adults younger than 40 years do not usually present with a second malignancy.[5] This case is unique as he presented at an age <40 years.
CASE REPORT
A 34-year-old male smoker, gutkha chewer, and chronic alcoholic patient presented with a painful non-healing ulcer on the right lateral margin of the tongue of 3-month duration with associated pain in the right side of face and ear and difficulty in eating and speaking aggravating for the past 1 month. On local examination, there was an irregular, non-bleeding, reddish-white, tender ulceroproliferative lesion of 4x3 cm size involving posterior part of the right lateral border of tongue extending to floor of mouth just short of tonsillolingual sulcus (alveolus free) [Figure 1]. On neck examination, the right-sided level II lymph nodes were palpable.

- Naked eye view of the ulceroproliferative lesion located on the right lateral border of tongue
Metastatic workup with US whole abdomen and chest X-ray posteroanterior view was normal. Contrast-enhanced computed tomography face and neck showed well-defined heterogeneously enhancing mass (1.9 × 1.2 cm) involving the right lateral border of tongue along with subcentimeter bilateral level II neck nodes [Figures 2a-c]. Biopsy from tongue lesion showed well-differentiated squamous cell carcinoma [Figure 3]. The hemogram showed leukocytosis 96.45 × 109/L (predominant neutrophilia with shift to the left) and blasts 2%, platelets 513 × 109/L, and occasional hypersegmented neutrophils. Bone marrow aspiration was hypercellular for age with predominance of myeloid series cells (M/E ratio = 7:1), 39% immature cells including 4% blast cells. Bone marrow biopsy was hypercellular for age with predominance of myeloid series cells suggestive of CML in blast crisis [Figure 4]. BCR-ABL translocation was positive in 11% of metaphases analyzed by GTG banding (G-banding by trypsin using Giemsa) [Figure 5]. He was diagnosed as a case of synchronous carcinoma right lateral border of tongue cT2cN1cM0 with CML (Philadelphia positive).
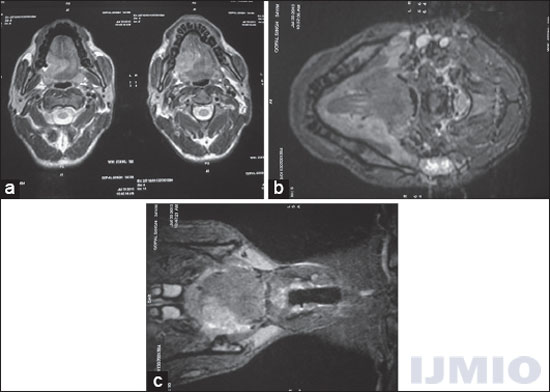
- Contrast-enhanced computed tomography scan of face and neck (a) axial view shows an enhancing lesion along the right lateral border of tongue crossing midline. (b) Axial view showing bilateral subcentimeter level II lymph nodes. (c) Coronal view of the same lesion involving intrinsic muscles of tongue

- Biopsy from tongue lesion showing features of well-differentiated squamous cell carcinoma (H and E stain, ×10) (Acknowledgment: Asmita Parhar, Anil Arora, and V K Arora, Department of Pathology, GTB Hospital and UCMS, Delhi)
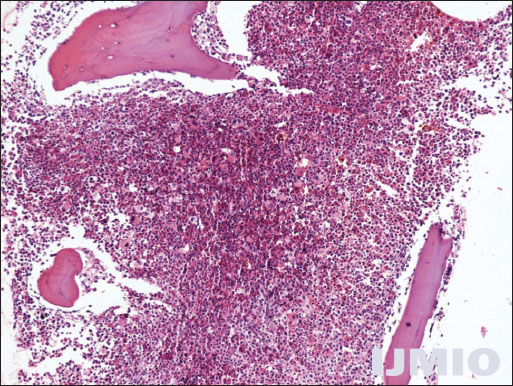
- Bone marrow biopsy showing predominance of myeloid series (H and E stain, ×10) (Acknowledgment: Asmita Parhar, Anil Arora, and V K Arora, Department of Pathology, GTB Hospital and UCMS, Delhi)
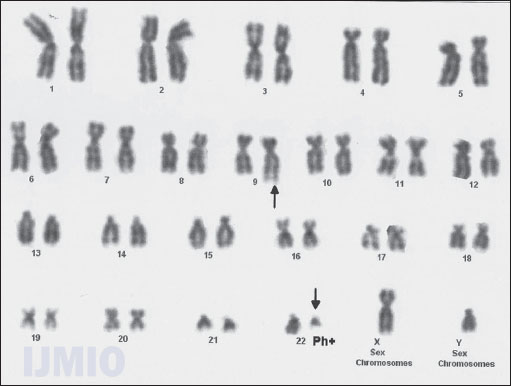
- G-banding by trypsin using Giemsa shows reciprocal translocation between chromosomes 9 and 22 (Philadelphia Positive) (Acknowledgment: Reita Ghosh, Double Helix, Clinical Cytogenetics and Reproductive Immunology Center, Delhi)
He was planned and started on concurrent chemoradiation to face and neck along with tablet Imatinib 400 mg once a day. He received external beam radiation by shrinking field technique to a dose of 70 Gy/35#/>7 weeks with gap correction along with concurrent Cisplatin 50 mg IV weekly. During the treatment, he was managed for mucositis and dermatitis. The patient has shown complete clinical response at the primary site and advised to follow-up regularly on outpatient basis.
DISCUSSION
The patient with one malignancy has increased the risk for another malignancy. The etiological factors contributory to association are positive family history, prior history of malignancy, immunologic and genetic defects, prolonged exposure to carcinogens, radiation and chemotherapy for the primary cancer, smoking and chemotherapy for the primary cancer, and smoking and alcohol. In this patient, a history of smoking seems to be significantly associated with both malignancies.
However, the study of factors at molecular level could further determine the causal factors (namely GTG banding in a case of CML).
This patient was treated conservatively keeping organ preservation in mind. He responded well to treatment and had shown complete response at the primary and nodal site. For his leukemic component, he was given Imatinib. The patient is kept on follow-up and expected to report timely for his next visit.
AUTHORS’ CONTRIBUTIONS
Sajal Goel Group 1 - Conception and design, acquisition of data, and analysis and interpretation of data. Group 2 - Drafting the article and critical revision of the article. Group 3 - Final approval of the version to be published. Deepak Kumar Mittal Group 2 - Drafting the article and critical revision of the article. Group 3 - Final approval of the version to be published. Pankaj Sharma Group 2 - Drafting the article and critical revision of the article. Group 3 - Final approval of the version to be published.
Acknowledgment
The authors acknowledge Dr. Parihar Asmitar, Dr. Arora Anil, Dr. Arora V K, and Dr. Ghosh Reita for pathological diagnosis.
REFERENCES
- Synchronous primary malignancies in breast and kidney: A rare case report. Indian J Surg. 2015;77:6-9.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical features of multiple primary malignancies: A retrospective analysis of 72 Chinese patients. Asian Pac J Cancer Prev. 2014;15:331-4.
- [Google Scholar]
- Gastric carcinoma and other malignancies in patients with chronic myelogenous leukemia. Case report and review of the literature, with particular reference to young adults. Johns Hopkins Med J. 1980;147:213-6.
- [Google Scholar]
- Synchronous carcinoma breast with chronic myelogenous leukemia: A rare presentation. Indian J Cancer. 2010;47:477-9.
- [CrossRef] [PubMed] [Google Scholar]




